Recent comments in /f/askscience
swami78 t1_j21f2bs wrote
Reply to comment by WilliamMorris420 in What is the ‘widest’ ancestral generation? by vesuvisian
I was hoping someone would do the math! Thanks.
Embarrassed_Roof_344 t1_j21exl9 wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Has anyone constructed an "anatomy of learning", linking all of the pedagogy paychology and neuroscience into a coherent structure?
MrMobster t1_j21es5j wrote
Reply to comment by tjernobyl in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Quite possible. Deictic reference (words that refer to people or places related to some universal viewpoint, usually the speaker) is central, very commonly used function of the human language. It would make sense that the language started with the desire to express these kind of relations.
Of course, there is no way to prove it as we have no way of knowing what the earliest languages looked like. I’m sure however it had a word that sounded something like “ma” or “pa” and referred to a close person or group of people.
[deleted] t1_j21efzg wrote
Reply to comment by islandsimian in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
[removed]
MrMobster t1_j21e5sv wrote
Reply to comment by PeanutSalsa in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Learning Hebrew ;)
I was lucky to have had an opportunity to study Old Testament Hebrew in school. It was in part what got me interested in theoretical linguistics.
MrMobster t1_j21dvb7 wrote
Reply to comment by SereneDreams03 in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Neither “dialect” nor “language” are strictly defined concepts in linguistics. The classical criterion of recognizing dialects is mutual intelligibility (the varieties are clearly different but people can understand each other), but it’s not entirely unproblematic. “Language” is usually recognized on the basis of some political, cultural or historical significance.
The current approach in linguistics is to leave these things somewhat ambiguous and just note different varieties and their relationship between each other (approach that glottolog takes). Some have been advocating for “doculects” - identifying a variety on the basis of the publication or data that describes it. In the end, one can come up with multiple different measures for what’s a dialect and what’s a language, many of them useful in own way. ,
Exceedingly t1_j21dkte wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Economics question on the current levels of inflation around the world: Milton Friedman once gave this response to the cause of inflation, stating it primarily caused by governments printing money via central banks.
> "Consumers don't produce it, producers don't produce it, the trade unions don't produce it, foreign sheikhs don't produce it, oil imports don't produce it. What produces it is too much government spending and too much government creation of money, and nothing else."
This makes sense to me as printing money dilutes the value of currency, making everything more expensive across the board rather than one specific sector.
Covid caused massive turmoil in March 2020 where indexes dipped more than in 2008, but it only lasted 1.5 months opposed to 2 years because this time governments started printing money to support markets, buying up bonds and other assets.
If you look at the balance sheets of these central banks it shows that they all printed hundreds of billions or even trillions of dollars just after March 2020, presumably to keep the markets afloat. Those balance sheets now show a strong correlation with current global inflation levels, just skewed a year or so.
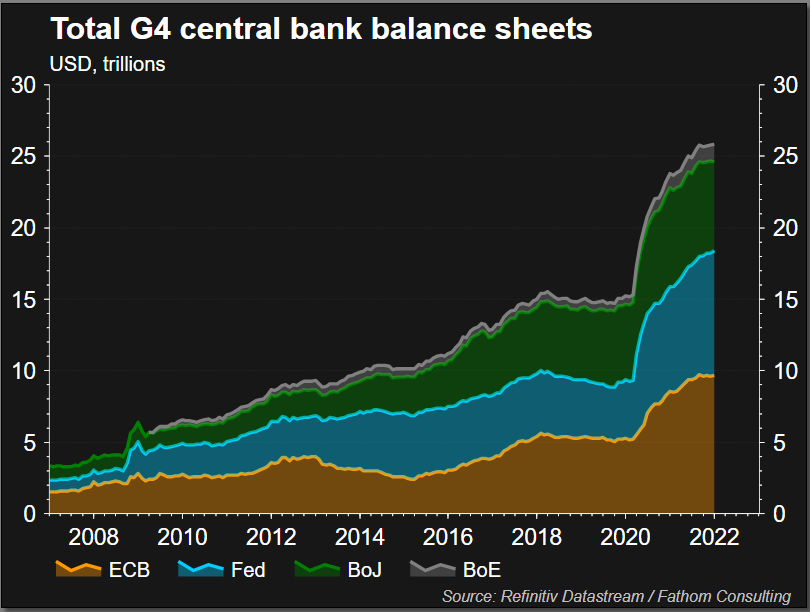{kind=link}
So is that it? Is the main cause of all this inflation just the knock on effect of governments spending their way out of a crash during covid? And if so, it's my understanding that the only way to truly reduce that inflation is to remove the printed money back out via a "market correction" period, aka a crash. Is that right? Insight from experts in the field would be welcome.
[deleted] t1_j21d5x4 wrote
Reply to comment by SpellingIsAhful in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
[removed]
DukeSuperior_Truth t1_j21d1m5 wrote
Reply to comment by przyssawka in How do shifts work on really long medical operations? by TerjiD
Exactly. Just because people can’t imagine doing something extraordinary, doesn’t mean it’s crazy or dangerous. People do ultramarathons that run 36 hours with no sleep as well. Adaptation is the operative word here.
[deleted] t1_j21cyke wrote
Reply to comment by AudienceRemote5915 in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
[removed]
bigharrydong t1_j21cfjh wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Can you explain to me why China has multiple PYRAMIDS throughout the countryside(that have been hidden by the CCP) and why they have Caucasian mummies inside of them?
bigharrydong t1_j21c5fu wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Can you explain to me why ancient "Egyptians" have Caucasian DNA?
bigharrydong t1_j21btat wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Can you explain to me what NAKED SHORTING is?
chazwomaq t1_j21bjxj wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
What is the best / most widely accepted / simplest model of political orientation? The left/right dimension is well known, and popular online systems like political compass add an authoritarian/libertarian dimension to make a 2D model.
What does the academic literature say? Specific references sought, preferably.
chazwomaq t1_j21b9tr wrote
Reply to comment by lcenine in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
We would call that a "cue" in psychology, although that term is not specific to the visual domain.
jbeansyboy t1_j21b0ez wrote
Reply to comment by Purecasher in How do shifts work on really long medical operations? by TerjiD
I tend to agree with most of what Vanilla says. I’m a relatively new private practice general surgeon and I’ll tell ya, I wish I had more time in residency, or at least more time for what I do.
I trained in the days of the “80 hr work week”. All the older folks say they are much better than us because they worked 120 hrs, etc. I think they may have graduated slightly better at overall surgery because they didn’t have to deal with as much administration as we do and most things were operative back then, AKA trauma solid organ injuries, AAAs, or intraabdominal abscesses are a few quick things that come to mind vs now we nonop most of those things.
Additionally I think they had the confidence to think they were good to go after residency because they had more autonomy back then. Most hospitals require attendings in the room now vs back in the older days, residents could operate alone. The ACGME leaves it up to the attendings to allow residents to operate alone but the hospitals have rules that supercede that if more conservative.
This all being said my 80hr work week was never such. Always in the high 90s and on transplant in the low 100s. But we log it as 80. Because we don’t want to get in trouble or losing credentialing.
I would be in favor of lengthening residency with the last year kind of a…. Pseudo attending year where you can operate alone with someone in the hospital in case you need it. You run your own clinic, take your own call, etc. and then having less hrs per week.
But I don’t think I would be in favor of tacking on more years for that. I’d like to get rid of some of the basic science in medical school. I spent a year relearning basically everything I learned in undergraduate courses. That I never use now. I’d just put those things as prerequisites to medical school.
I’d also like to see more direct pathways to specialities ~5 years if one chooses. I do private practice MIS/gen surg. I spent many many many hours and days helping with liver and pancreas transplants that I do not feel help me on a regular basis, or ever. Maybe see a few but not spent 20 weeks on the service. That time could have been seeing and doing more bread and butter surgical cases. Same with endovascular and etc. vascular and CTS are moving toward this.
For those that aren’t sure what they want to do they would have to finish formal residency and then do fellowship like we currently have.
For things like family medicine, emergency medicine, peds, and derm, it already seems very doable how it’s set up. They didn’t seem to work many hrs at all given how their speciality. Good for them!
tjernobyl t1_j21avnp wrote
Reply to Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Did the earliest languages have pronouns?
xlnfraction t1_j218u3u wrote
Reply to comment by OakBayIsANecropolis in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Also them criticizing sapiens is rly fun to read tbh (and pretty true lol)
JewishSpaceTrooper t1_j218mko wrote
Reply to comment by wishingtoheal in How do shifts work on really long medical operations? by TerjiD
ABSOLUTELY 💯 agree!!! The for-profit institutions, specifically the Nurse Practitioner schools, that, for the sake of aforementioned profit, have dropped pre-requisite skills and experience, to virtually the bare minimum. And, let’s not mention the ONLINE education slide (of abomination) from BSN to NP…how the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN) signed off on this is beyond me. Soon enough, the poor people in this country, will only see a physician very rarely….while NPs already handle cases far too complicated for their expertise. What a time to be alive
[deleted] t1_j216rze wrote
Reply to comment by TheRomanRuler in How do shifts work on really long medical operations? by TerjiD
[removed]
Kael_Doreibo t1_j216kom wrote
Reply to comment by TheRomanRuler in How do shifts work on really long medical operations? by TerjiD
Your biggest problem with this, particularly in the emergency departments, is the sudden onset of emergencies, their scale, and the time needed for certain surgeries/procedures. There are times when you, as a medical practitioner, need to be on for the entire period that it takes to resolve the onset of cases before you because any switch-over will result in loss of information and potentially death. With so many emergencies happening all the time in a larger population/operational radius of the hospital it become untenable to keep to that kind of schedule consistently and any inconsistencies results in a cascade effect across rosters/schedules.
It's good to at least attempt to keep to that kind of schedule and it makes sense to try it at least but ultimately it is impossible to just say "this is the solution" for every scenario.
KWillets t1_j2163iy wrote
Reply to comment by Akagiyama in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
Yes, second language learning difficulty is measured relative to the first language.
The US DLI and state department difficulty rankings are based on the number of hours for an English speaker to learn the target language; it's different for speakers of other languages. For instance Korean speakers have little trouble with Japanese, despite these being category IV (hardest) on the DLI scale.
Factors that make languages easy or hard are vocabulary, grammar, reading and writing system, and cultural cues (and a few others that I can't recall at the moment). Category IV languages have differences from English in all of these categories.
[deleted] t1_j215iyy wrote
Reply to comment by Wireeeee in How do shifts work on really long medical operations? by TerjiD
[removed]
JewishSpaceTrooper t1_j215fpa wrote
1.) TRIAGE: complicated emergency cases, that may need long-haul surgical intervention, get triaged to the best equipped hospital (often a teaching facility) with lots of highly experienced staff. 2.) these large institutions, each State usually has several large medical teaching hospitals, don’t just employ General Surgeons. These lovely places will provide several sub-specialty doctors depending the need and often include vascular surgeons, orthopedic surgeons (often with a sub-sub specialty in pelvic or shoulder injuries), plastic surgeons, neurosurgeons and the list goes on and on. I’ve literally seen long-haul surgeries that necessitated 5 different surgeons to go in, with two scrubbing in, and one finishing up his/her part. 3.)Surgical techs/nurses usually work on strict 12 hour rotations, especially if they’re unionized. So these guys/gals are never really ever in need to work to sheer exhaustion. Well, at least time wise….I’ve seen some nurses/techs literally be stomped into the ground by dipshit surgeons, but that’s another story.
So, in today’s environment, the overworked-heroic surgical staff trope, isn’t a thing any more. You have to be in extremely remote places where even helicopters can’t triage an unfortunate soul. Lord have mercy in most places if Dr. “Neurosurgeon” is going to miss his soirée or golf game due to an unforeseen complication….Anyways, all of the above are good things! You DO NOT want anyone performing surgery for longer than 8 to max 10 straight hours. Even Mr. Big Brain Neurosurgeon with his/her extra-long fellowship declines rapidly after 7 hours. Disclaimer: Yes, yes….this Redditor may be partial toward the great field of Neurosurgery, and the big-headed minions that staff this hallowed field.
UpsideVII t1_j21g6nj wrote
Reply to comment by ejMileman in Ask Anything Wednesday - Economics, Political Science, Linguistics, Anthropology by AutoModerator
The market does set the (long-run) price for money.
The price of money is the real interest rate which is the nominal interest rate (managed by the fed) minus inflation (determined by the market). If the fed tried to perpetually lower the nominal rate, this will lead to higher inflation (assuming nothing else is changing) as the market restores the "natural" real interest rate.
The reason we do this is because highly variable inflation in very costly. For example, it makes it risky to lend money (as you don't know if the money will be worth much less when you get paid back due to a large bout of inflation) which makes it costly for businesses to raise capital and depresses the economy.
By manipulating the nominal rate so that it "absorbs" all the market fluctuations in demand for money (which cause variation in the real rate), the fed is able to maintain a low, stable inflation level and eliminate this problem. This is why you will sometimes hear about the fed's "inflation target" and why we find it optimal to have an entity managing the money supply.